Dental X-Ray Systems: Technology, Performance, Types (IOPA, OPG, CBCT) & AERB Regulatory Compliance Guide
Comprehensive guide to dental X-ray systems including IOPA, panoramic (OPG), CBCT and handheld dental X-ray units. Learn technical specifications, radiation safety, QA standards and AERB licensing requirements for dental clinics in India.
HOT X-RAY PRODUCTS
3/6/20264 min read


The Comprehensive Guide to Dental X-Ray Systems: Technology, Performance, and AERB Regulatory Compliance
The evolution of dental diagnostic imaging has progressed from the first crude dental X-ray taken by Otto Walkhoff in 1896 to today’s high-precision, digital, and even handheld systems. For modern dental clinics, choosing the right X-ray modality—whether it is Intra-Oral Peri-Apical (IOPA), Ortho Pantomography (OPG), or Dental Cone Beam Computed Tomography (CBCT)—is a balance of clinical utility, image resolution, and strict adherence to the Atomic Energy Regulatory Board (AERB) safety standards.
Types of Dental X-Ray Systems
Under AERB safety codes, dental X-ray equipment is categorized based on its diagnostic application and portability:
Intra-oral Peri-apical (IOPA): These units are used with intra-oral films or digital sensors. They can be wall-mounted, stand-mounted, or handheld.
Panoramic Radiography (OPG): These provide a broad view of the entire jaw, teeth, and joints.
Dental Cone Beam CT (CBCT): A high-resolution 3D imaging modality used for implants and complex surgeries.
Handheld/Portable Units: Defined as equipment intended to be carried by one or two persons and must not exceed 12 kg in weight.
Technical Specifications & Performance Benchmarks
The diagnostic efficacy of a dental X-ray system depends on several internal technical parameters. Recent independent studies comparing handheld units (like the Nomad Pro) to traditional wall-mounted sources (like the Planmeca Intra) reveal critical performance differences:
Operating Potential (kVp) and Tube Current (mA)
Wall-Mounted Units: Typically operate at a constant potential of 70 kVp and 8 mA.
Handheld Units: Often operate at a constant potential of 60 kVp and 2.5 mA. The lower mA in handheld units is compensated for by optimized exposure times and closer proximity to the patient.
Focal Spot and Image Resolution
A critical benchmark for image detail is the Line Pair (LP) resolution. Research shows that handheld devices often provide significantly higher mean LP resolution (6.05–6.55 lp/mm) compared to wall-mounted sources (5.58–6.31 lp/mm). This is largely due to the smaller focal spot size found in handheld units (0.4 mm) versus traditional units (0.7 mm).
Source-to-Skin Distance (SSD)
AERB mandates specific minimum distances to protect the patient:
For units operating above 60 kVp and up to 75 kVp, the minimum focus-to-skin distance must be 20 cm.
For units operating above 75 kVp, the distance must be at least 30 cm.
Dosimetry: Patient and Operator Safety
Radiation safety is governed by the ALARA (As Low As Reasonably Achievable) principle.
Patient Dose Reduction
Optimizing exposure factors can lead to dramatic reductions in patient dose. One study recorded that the mean effective dose for a Full Mouth Examination (FMX) was significantly less for handheld devices (36 µSv) than for wall-mounted devices (98 µSv). This represents a total effective dose reduction of approximately 12% when transitioning to optimized handheld technology.
Operator Protection
Operators are mandated to follow strict safety protocols:
Lead Aprons: Must be worn by operators, especially when using mobile or portable units, and must have a minimum lead equivalence of 0.25 mm.
TLD Badges: Every radiation worker must use personnel monitoring services (TLD badges). The badge should be worn below the lead apron and stored in a radiation-free zone when not in use.
Dose Limits: The effective dose for occupational workers must not exceed 20 mSv averaged over five years, or 30 mSv in any single year.
Regulatory Framework in India (CDSCO and AERB)
Every dental practitioner in India must navigate two distinct regulatory paths to operate X-ray equipment legally.
CDSCO Classification
As of January 1, 2021, all X-ray machines are classified as Class C (Moderate to High Risk) medical devices. Registration with the Central Drugs Standard Control Organization (CDSCO) is mandatory for any legal manufacture or import to prevent the use of inferior quality products that could lead to misdiagnosis.
AERB Licensing via e-LORA
No diagnostic X-ray equipment can be used for patient diagnosis until a Licence for Operation is obtained through the AERB’s e-LORA (e-Licensing of Radiation Applications) portal.
The Step-by-Step e-LORA Process for Dental Users:
Institute Registration: Register your clinic/institute on the e-LORA website.
Procurement Permission: Apply for permission to procure an AERB Type Approved model from an authorized supplier.
Installation & QA: Once the unit is delivered, it must be installed by an authorized engineer, and a Quality Assurance (QA) check must be performed.
License Application: Fill out the Application for Registration/License, upload the QA report and installation report, and wait for AERB approval.
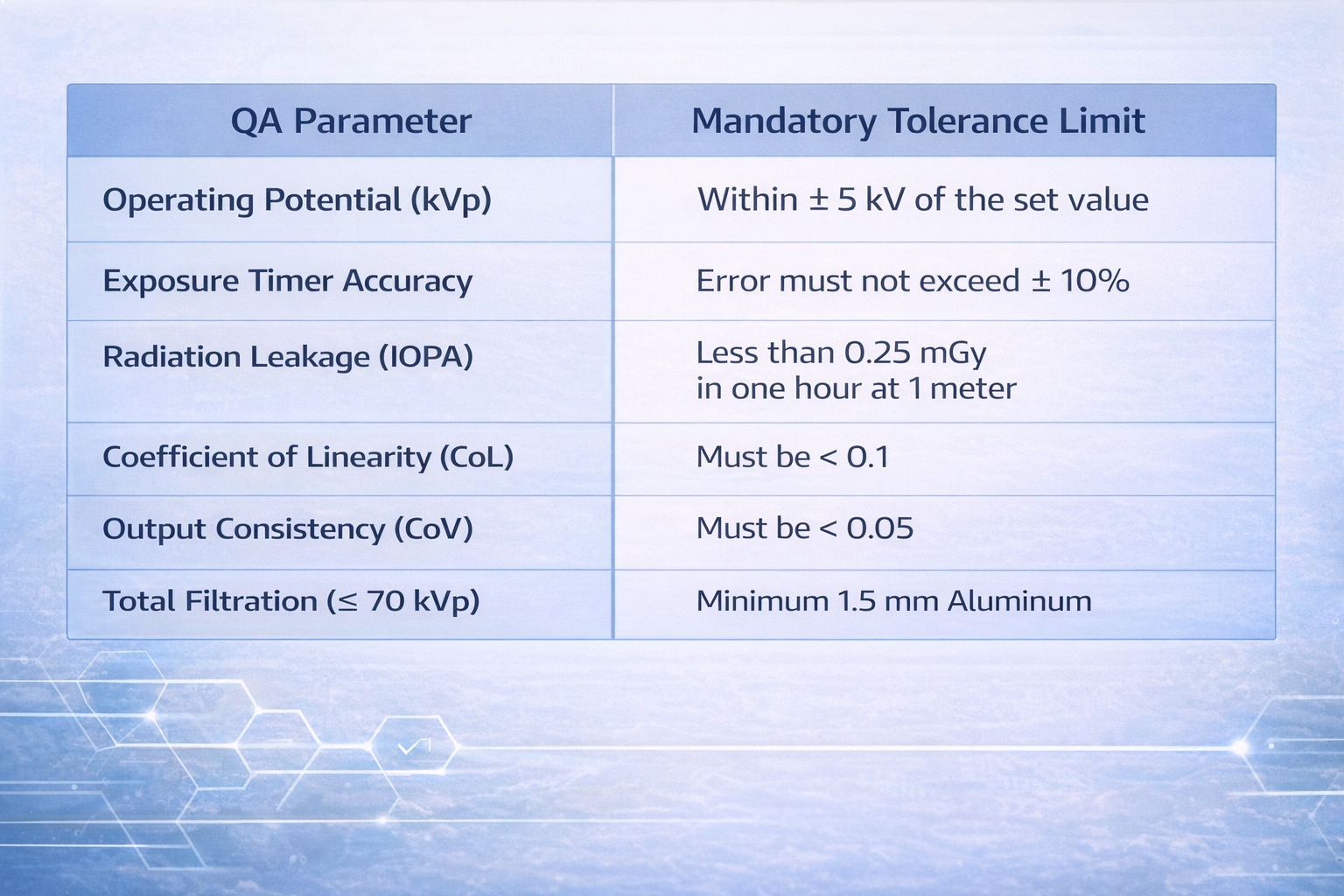
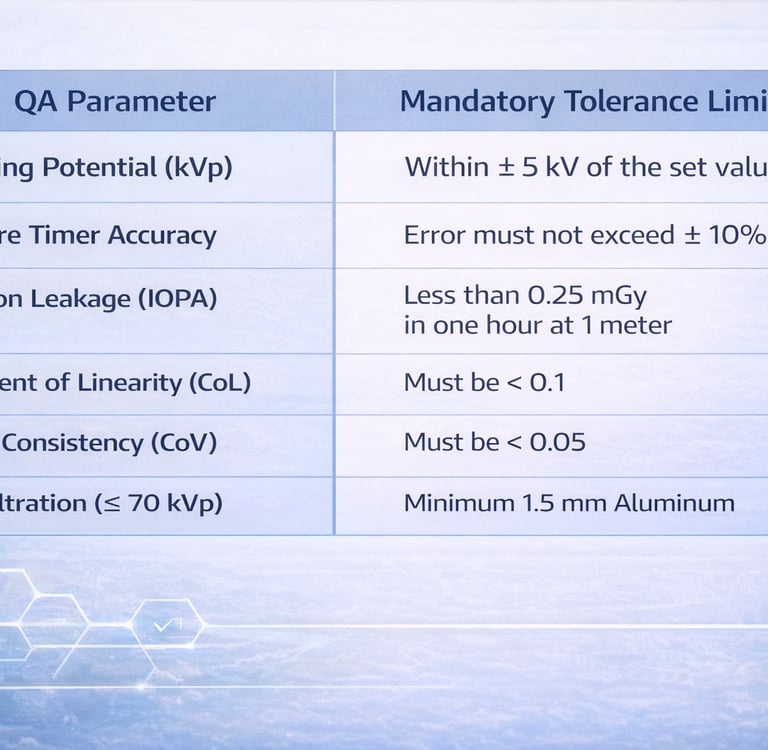
Quality Assurance (QA) Standards
AERB requires that periodic QA be carried out by authorized agencies every two years, or after major repairs, to ensure the equipment meets safety benchmarks.
Operational Best Practices & Staffing
For a dental facility to remain compliant, it must meet specific staffing and shielding requirements:
Qualified Personnel: Installations must have a radiologist, related medical practitioner, or X-ray technologist pass from a recognized institution to operate the equipment.
Shielding: Walls, doors, and floors of the X-ray room must have appropriate structural shielding. For example, all doors should have a lead lining of 1.7 mm.
Room Layout: The room must be large enough to facilitate easy staff movement and proper patient positioning. A permanent radiation warning symbol must be posted on the entrance door.
Holding Patients: Operators should avoid routinely holding patients. If an assistant must hold a child or infirm patient, they must wear a lead apron.
Conclusion
Dental X-ray systems are "hot products" for a reason—they offer incredible resolution and clinical flexibility. However, as noted by researchers, while the technology simplifies the diagnostic task, it increases the operator’s proximity to the source. Achieving clinical success with these systems requires more than just procurement; it demands a deep commitment to AERB guidelines, consistent Quality Assurance testing, and a culture of safety that protects both the patient and the healthcare professional.
About XRAYNEWS.NET
XRAYNEWS.NET provides updates on medical and industrial X-ray technologies, radiography insights, regulatory awareness, and imaging industry developments.
Regulatory Resources
© 2025. All rights reserved.
Video Resources
Popular Topics
Quick Links
Stay Updated with X-Ray Industry News
Subscribe to receive updates on X-ray technology developments, radiography insights, and industry news.