Mobile X-Ray Units: Technology, Specifications, QA Testing & AERB Regulatory Compliance Guide
Mobile X-ray units enable bedside radiography in hospitals, ICUs, and emergency wards. Learn about technology, performance benchmarks, QA testing standards, and AERB regulatory compliance requirements in India.
HOT X-RAY PRODUCTS
3/6/20265 min read
The Definitive Guide to Mobile X-Ray Units: Technology, Performance, and AERB Regulatory Compliance
In the fast-paced environment of modern hospitals, diagnostic speed and patient comfort are paramount. Mobile X-ray units have become an indispensable "hot" product category for xraynews readers, bridging the gap between high-powered fixed installations and ultra-portable handheld devices. Designed to be wheeled directly to the bedside in ICUs, emergency rooms, and wards, these units are critical for patients too unstable for transport. However, their use is governed by a rigorous technical and regulatory framework defined by the Atomic Energy Regulatory Board (AERB) and the Central Drugs Standard Control Organization (CDSCO) in India.
Defining Mobile X-Ray Equipment
According to the AERB Safety Code (AERB/RF-MED/SC-3), mobile X-ray equipment is specifically defined as equipment intended to be moved from one location to another between periods of use while supported by its own wheels or equivalent means of support, without dismantling, for use within a single institution.
A vital regulatory distinction for healthcare providers is that the movement of mobile X-ray equipment is restricted within the institution for which it is registered. If a unit is intended to be carried by one or two persons and weighs less than 12 kg, it is classified as "Portable," which has different movement allowances.
Technical Specifications and Design Requirements
Mobile units are engineered to provide diagnostic power comparable to fixed room installations while maintaining maneuverability. High-frequency generators are standard, ensuring stable radiation output and reducing patient dose through optimized exposure factors.
Key Performance Benchmarks
Operating Potential (kVp) and Tube Current (mA): Mobile units typically operate at higher potentials than handheld units. While a handheld device like the Nomad Pro operates at a constant 60 kVp and 2.5 mA, mobile units often range up to 100–125 kVp with significantly higher mA ratings to capture clear images of thick body parts like the chest or abdomen.
Effective Focal Spot Size: The ability to resolve small details (image resolution) depends heavily on the focal spot size. While high-end mobile units aim for small focal spots (e.g., 0.6 mm to 1.0 mm), studies show that even smaller spots (0.4 mm) in handheld units can lead to higher Line Pair (LP) resolution.
Total Filtration: To protect patients, AERB mandates that the total filtration in the primary beam must be at least 2.5 mm Al equivalent for units operating at a constant potential. This cuts off low-energy radiation that does not contribute to the image but increases the patient’s absorbed dose.
Tube Housing and Leakage: The X-ray tube housing must be constructed so that leakage radiation in any direction does not exceed 1 mGy in one hour at a distance of 1.0 meter from the focus when operating at its maximum rated parameters.
Operational Safety: The TDS Principle
Safety in mobile radiography is built on the Time-Distance-Shielding (TDS) principle to ensure exposures remain ALARA (As Low As Reasonably Achievable).
Mandatory Operator Protection
Exposure Cable Length: AERB design requirements state that for mobile radiography units, the exposure cable length must not be less than 2 meters. This allows the operator to stand at a safe distance from the radiation source and the patient (the primary source of scatter) during the shot.
Lead Aprons and Accessories: It is mandatory for operators to wear a lead apron with a minimum of 0.25 mm lead equivalence. For high-volume environments, mobile protective barriers (MPB) with a minimum of 1.5 mm lead equivalence and a viewing window should be utilized.
Safe Distance and Scatter: Research indicates that the highest scatter dose is observed in the direction back towards the X-ray tube (180°). For high-volume screening (e.g., 50+ exams/day), maintaining a distance of at least 2.5 to 4.5 meters is recommended to stay below the public dose limit of 1 mSv/year.
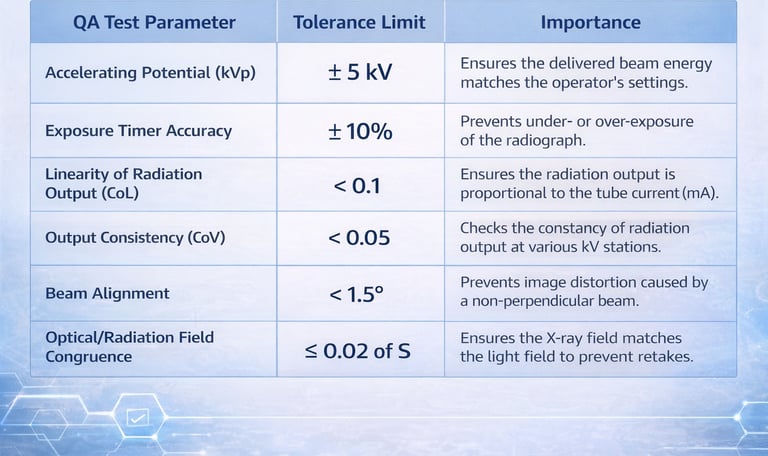
Quality Assurance (QA) Benchmarks
To ensure the equipment performs satisfactorily and remains in compliance with safety standards, regular Quality Assurance (QA) tests are mandatory. These must be performed at the time of installation and repeated once every two years, or after any major repair.
5. Regulatory Framework in India
Procuring and operating a mobile X-ray unit involves navigating two primary regulatory bodies: the CDSCO and the AERB.
CDSCO Classification
Mobile X-ray machines are classified as Class C (Moderate to High Risk) medical devices. Mandatory registration with the CDSCO for the import or manufacture of these devices has been in effect since January 1, 2021. This regulation was implemented to prevent the proliferation of inferior quality or mis-branded products that could lead to misdiagnosis.
AERB and the e-LORA Portal
The AERB governs the radiological safety of the equipment through its e-LORA (e-Licensing of Radiation Applications) system. No unit can be legally used for patient diagnosis until a valid Licence for Operation is obtained.
Step-by-Step Licensing Process:
Institute Registration: The medical facility must register on the e-LORA portal using its official details.
Procurement Permission: The facility applies for permission to procure a specific AERB Type Approved model from an authorized supplier.
Installation and QA: Upon delivery, an authorized engineer installs the unit and a third-party agency performs the mandatory QA tests.
Licence Application: The facility uploads the Installation Report and QA Summary Report to e-LORA to apply for the final Licence for Operation.
Personnel Monitoring: TLD Badges
Every radiation worker operating a mobile unit is mandated to use Personnel Monitoring Services (PMS), typically through TLD (Thermoluminescent Dosimeter) badges.
Proper Usage: The TLD badge must be worn below the lead apron at the chest level to monitor the dose to the torso.
Storage: When not in use, badges must be stored in a radiation-free zone outside the X-ray room.
Dose Limits: The annual effective dose for occupational workers is 20 mSv, averaged over five years, with a maximum of 30 mSv in any single year.
Pros and Cons of Mobile X-Ray Units
Pros
Clinical Flexibility: Allows for immediate imaging of trauma, pediatric, or non-ambulatory patients without the risks associated with internal hospital transport.
High Power Efficiency: Unlike battery-limited handhelds, mobile units often have robust power systems capable of shorter exposure times, which reduces motion blur in images.
Integrated Workflow: Most modern units are fully digital, allowing for "instant" image review on a built-in workstation, which is vital in critical care decisions.
Cons
Institutional Constraints: Unlike truly portable units, mobile equipment is legally bound to the specific institution where it is licensed and cannot be taken to field camps or external clinics.
Space Requirements: While mobile, these units are heavy and require dedicated storage space that must be a "sanitary environment" free from dust and water leakage.
Regulatory Rigor: Because they are high-powered devices, they require the same level of QA and personnel monitoring as a fixed X-ray room, increasing the administrative workload for the facility.
Conclusion
Mobile X-ray units represent a pinnacle of diagnostic convenience for modern medical facilities. Their status as a "hot" product is justified by their ability to provide high-resolution imaging at the point of care. However, for a facility to be successful and safe, it must go beyond simple procurement. True excellence in mobile radiography requires a deep commitment to AERB compliance, meticulous Quality Assurance, and a culture of ALARA-based safety that protects both the patient and the dedicated healthcare professionals operating the equipment.
About XRAYNEWS.NET
XRAYNEWS.NET provides updates on medical and industrial X-ray technologies, radiography insights, regulatory awareness, and imaging industry developments.
Regulatory Resources
© 2025. All rights reserved.
Video Resources
Popular Topics
Quick Links
Stay Updated with X-Ray Industry News
Subscribe to receive updates on X-ray technology developments, radiography insights, and industry news.