Computed Radiography (CR) vs Digital Radiography (DR): Key Differences, Benefits & AERB Compliance Guide
Compare CR vs DR systems in X-ray imaging with detailed insights on technology, workflow, dose efficiency, and AERB compliance for modern radiology facilities.
INDUSTRY INSIGHTS & TECHNOLOGY
3/17/20264 min read
Computed Radiography (CR) vs. Digital Radiography (DR): A Technical and Regulatory Comparison for Modern X-Ray Facilities
The transition from traditional film-based imaging to digital modalities has revolutionized medical and dental diagnostics by aiming at the optimization of image quality and patient dose. Within the digital landscape, two primary technologies dominate: Computed Radiography (CR) and Digital Radiography (DR). While both systems fulfill the objective of producing high-quality diagnostic information, they differ fundamentally in their technological foundation, workflow efficiency, and maintenance requirements as mandated by the Atomic Energy Regulatory Board (AERB).
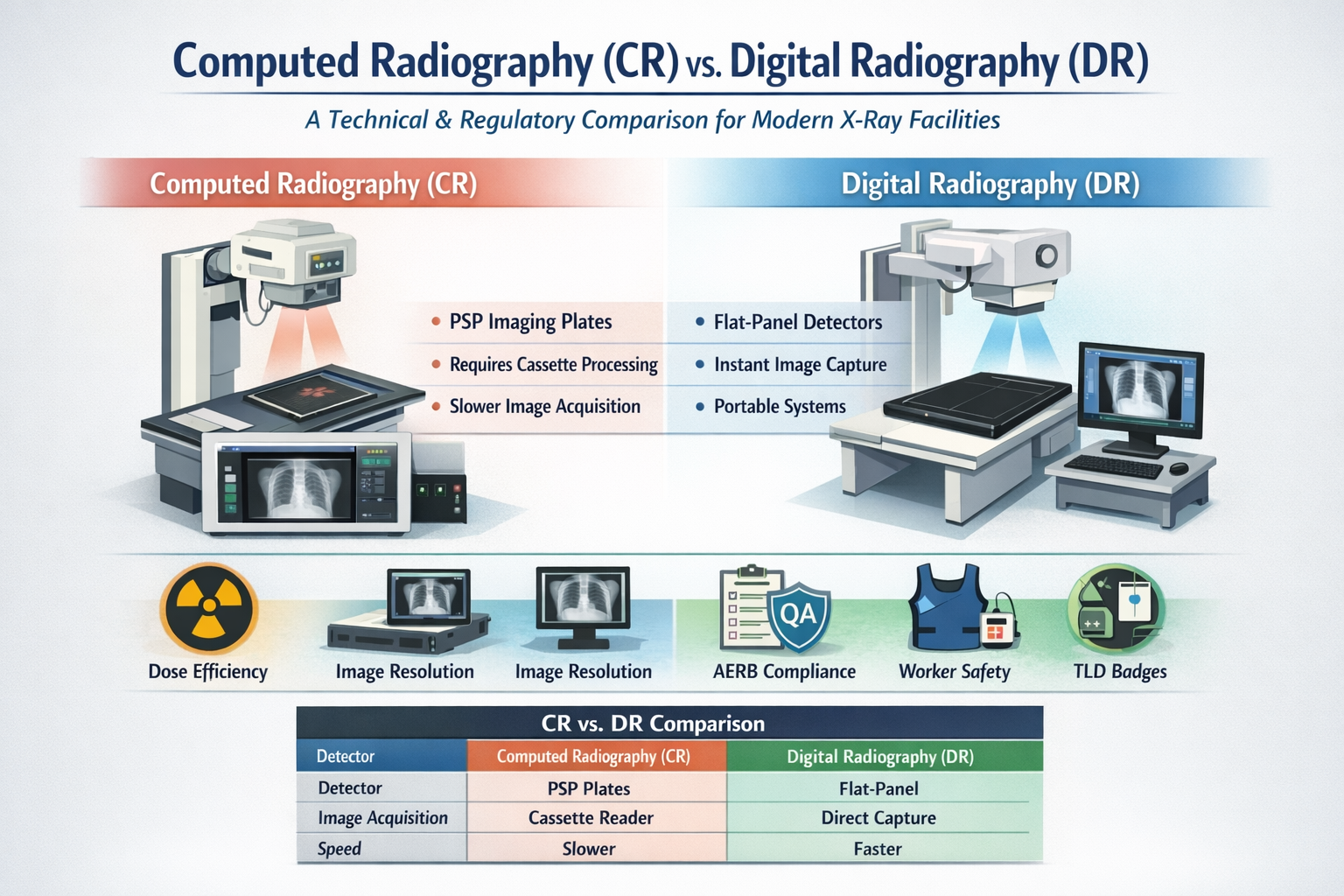
1. Technological Foundations: PSP vs. Flat-Panel Detectors
The primary distinction between CR and DR lies in the "Imaging Device," defined by the AERB as a detector unit or array of detectors that receives X-rays and produces an electrical or light signal.
Computed Radiography (CR) utilizes Photostimulable Phosphor (PSP) imaging plates. In a CR workflow, the X-ray energy is captured as a latent image on a phosphor plate housed within a cassette. This cassette is then physically transported to a reader unit, where the information is scanned (typically at resolutions like 300 to 600 dots per inch) to produce a digital image. The sources note that scanning at 300 DPI can approach the theoretical threshold for resolution, suggesting that higher DPI settings may be required for finer detail.
Digital Radiography (DR), often called "direct digital," employs flat-panel detectors that convert X-rays directly into digital signals without a secondary scanning step. Modern ultraportable systems often utilize highly sensitive and dose-efficient LG Oxide Detectors (e.g., 14” x 17” panels) that provide near-instantaneous visualization on a laptop or portable workstation.
2. Performance Benchmarks and Image Resolution
A critical performance benchmark for any imaging system is its Line Pair (LP) resolution, which measures the ability to visualize small anatomical details.
Resolution Comparisons: Research into intraoral radiography shows that digital systems can offer superior detail compared to traditional sources. Studies comparing handheld devices (using PSP) to wall-mounted sources found that handheld units achieved significantly higher mean LP resolution (6.05–6.55 lp/mm) compared to fixed units (5.58–6.31 lp/mm). This superiority is primarily attributed to a smaller focal spot size (0.4 mm) in the handheld unit versus 0.7 mm in fixed units.
Contrast Benchmarks: AERB Quality Assurance (QA) standards mandate that imaging systems resolve specific patterns. High Contrast Resolution must resolve a mesh pattern of 30 lines/inch or a bar pattern of 1.5 lp/mm. Low Contrast Resolution requires the visualization of a 3.0 mm hole pattern to ensure that structures differing slightly in radio-opacity are detectable.
3. Dose Efficiency and Patient Safety
One of the most significant advantages of digital modalities is the potential for patient dose reduction through the optimization of exposure factors.
Comparative Dosimetry: Clinical simulations of a Full Mouth Examination (FMX) revealed that using optimized digital protocols resulted in a mean patient dose of 36 µSv for handheld units, significantly lower than the 98 µSv recorded for wall-mounted devices. This represents an effective dose reduction of approximately 12%.
Sensitivity: Digital detectors, particularly modern oxide-based DR panels, are designed to be "highly sensitive," allowing for diagnostic images at lower radiation levels. However, because portable systems often lack Automatic Exposure Control (AEC), operators must manually adjust the tube current (mA) and exposure time (mAs) based on patient size to prevent unnecessary exposure.
4. Workflow, Portability, and Clinical Application
The shift toward Digital Radiography (DR) has facilitated the development of ultraportable (UP) X-ray systems that can fit within a suitcase or backpack.
Field Use: UP systems are ideal for community-based screening, such as Tuberculosis (TB) programs. These systems pair a battery-powered X-ray tube with a DR detector and AI-powered Computer-Aided Detection (CAD) software. This combination allows for automated, standardized image interpretation in regions where expert human readers are scarce.
Speed: Unlike CR, which requires the manual handling of cassettes and a wait time for scanning, DR provides immediate feedback. This is vital in emergency operations, forensics, and humanitarian missions where access to traditional fixed infrastructure is unavailable.
5. AERB Regulatory and Quality Assurance (QA) Mandates
Regardless of the modality, all imaging systems must comply with AERB Safety Code AERB/RF-MED/SC-3 (Rev. 2).
Modality-Specific Maintenance:
CR Maintenance: CR plates must be periodically evaluated for artifacts, and the cleaning frequency must follow manufacturer-recommended procedures.
DR Maintenance: Digital detectors must be calibrated periodically as per manufacturer recommendations to maintain functional performance.
Periodic QA Testing: End-users are responsible for ensuring that periodic QA is carried out by authorized agencies at least once every two years, or after major repairs. Key QA parameters include:
Operating Potential (kVp): Must be within ± 5 kV of the set value.
Timer Accuracy: Exposure time error must not exceed ± 10%.
Radiation Leakage: For radiography units, leakage must not exceed 1 mGy in one hour at 1 meter from the focus.
Optical/Radiation Field Congruence: The discrepancy must be ≤ 0.02 of S (focal spot to image receptor distance) to prevent retakes.
6. Data Security and PACS Integration
To ensure diagnostic continuity, both CR and DR systems must be integrated into a secure digital environment.
Networking: Imaging devices interconnected by computer networks must exchange information in accordance with national and international standards to prevent the loss of patient data.
PACS: When using a Picture Archiving and Communication System (PACS), facilities must ensure that the quality of patient images is maintained and that information is not unintentionally altered during storage or transmission.
7. Occupational Safety and the Role of the RSO
While digital detectors reduce patient dose, the protection of radiation workers remains a priority, especially for handheld and portable units where the operator stands near the source.
Safety Tools: Operators are mandated to use personnel monitoring services (specifically TLD badges) and wear lead aprons with a minimum of 0.25 mm lead equivalence. TLD badges must be worn below the lead apron and stored in a radiation-free zone when not in use.
Staffing: Every facility must designate an AERB-approved Radiological Safety Officer (RSO). For high-risk facilities like CT and Interventional Radiology (IR), the RSO must be a radiologist or a technologist with at least three years of working experience in the field.
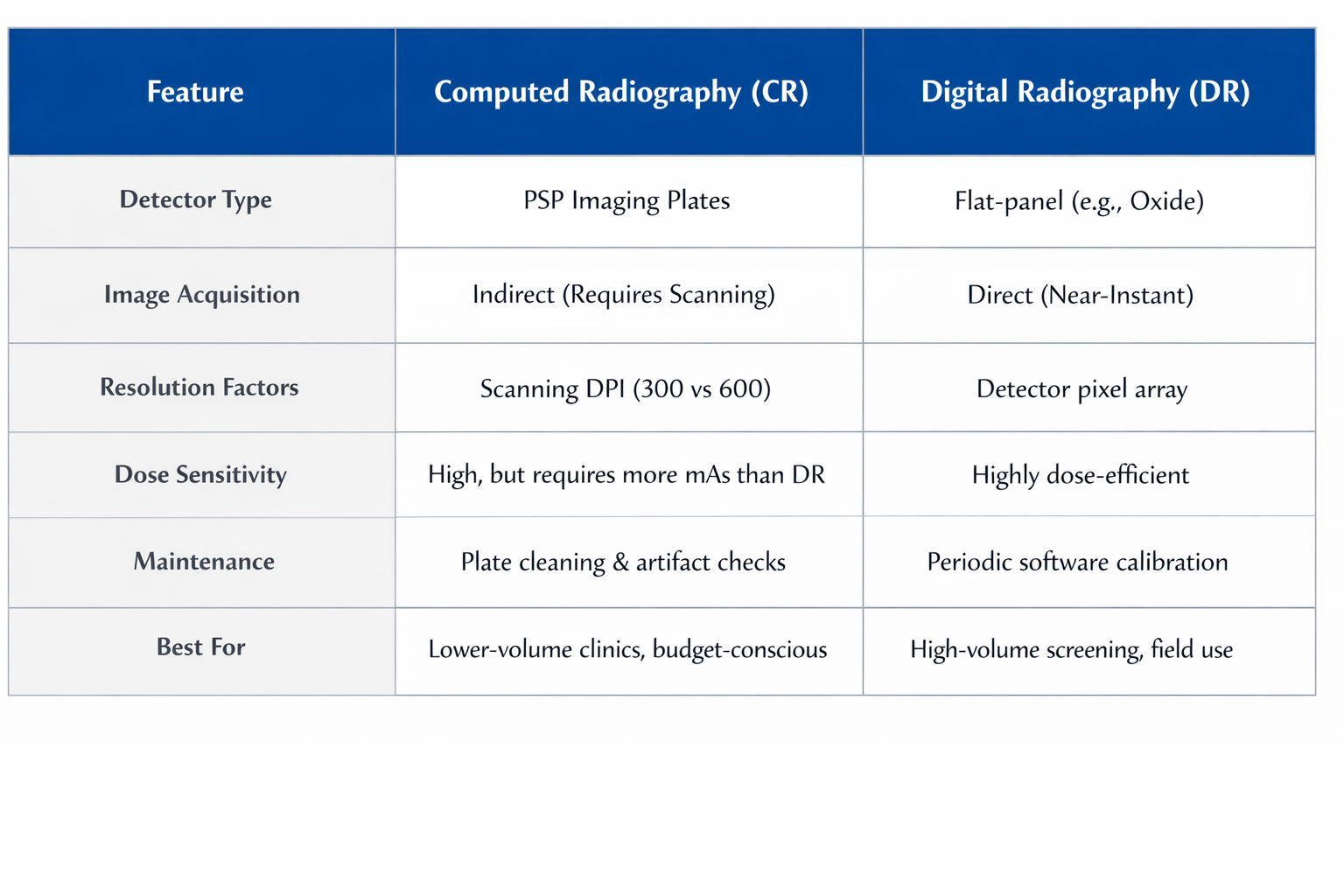
Summary of Comparison
Conclusion
Both CR and DR represent a significant leap from analog film, fulfilling the AERB’s mission to ensure that radiation risk to patients is minimized through optimization and justification. While CR systems remain a viable digital pathway through the use of reusable PSP plates, DR technology is the gold standard for modern workflow efficiency, particularly in ultraportable applications and AI-integrated screening programs. Clinical success with either modality requires a rigorous commitment to bi-annual QA testing, e-LORA licensing, and a culture of safety centered on the ALARA (As Low As Reasonably Achievable) principle.
About XRAYNNEWS.NET
XRAYNEWS.NET provides updates on medical and industrial X-ray technologies, radiography insights, regulatory awareness, and imaging industry developments.
Regulatory Resources
© 2025. All rights reserved.
Video Resources
Popular Topics
Quick Links
Stay Updated with X-Ray Industry News
Subscribe to receive updates on X-ray technology developments, radiography insights, and industry news.